
穴位刺激防治POGD的有效性逐渐被临床所认可。
术后胃肠功能障碍(postoperative gastrointestinal dysfunction,POGD)是指外科手术后受手术创伤、术中失血、麻醉药物等因素的影响,引起的以消化道症状为主的临床综合征。POGD以胃肠道运动功能障碍为主要特点,是外科手术后常见并发症之一,可导致患者住院时间延长、费用增加,同时其伴随的腹痛腹胀、恶心呕吐等症状给患者带来极差的主观体验。
POGD主要临床表现有恶心、呕吐、腹痛、腹胀、不耐受经口进食等,包括以术后恶心呕吐(postoperative nausea and vomiting,PONV)为主的上消化道症状和以术后麻痹性肠梗阻(postoperative ileus,POI)为主的下消化道症状。PONV是指术后至少有一次恶心、干呕或呕吐,或者以上症状的任何组合,多发生在术后24h内[2]。POI多发生于腹部大手术后,主要表现为延迟排气排便,伴有恶心呕吐、腹痛腹胀、肠鸣音消失,不耐受经口进食等,持续时间可长达3-7d。
根据术后快速康复理念的指导,主要采用药物疗法和非药物疗法防治POGD,且预防比治疗更重要。目前PONV防治指南和专家共识提出以术前评估PONV风险等级为基础,采用逐层分级、递增止吐药种类的药物防治方案[3]。随着止吐药物种类的增多,PONV发生率逐渐下降,每增加一种药物种类可使发病风险下降26%[4]。然而,高风险患者即使使用2~3类止吐药,PONV发病率仍高于20%,继续追加药物种类及剂量,也难以进一步降低PONV发生率,且副作用发生率大大增加[5]。POI的防治包括药物疗法和非药物疗法。目前的一线防治药物为促胃肠动力剂,如外周阿片受体阻滞剂、脑肽、胃动素、肾上腺素能拮抗剂和胆碱能药物等[6]。与安慰剂相比,单靶点促动力药不能改善排便和排气时间,却能诱发心血管不良反应和免疫抑制作用[7],因此单纯使用某一类药物治疗POI往往不能取得满意疗效。灌肠和泻药可促进患者快速排气排便,但只是暂时缓解POI症状,并不利于胃肠功能的恢复。此外,它们还会刺激胃肠道,极大地增加电解质紊乱的风险。其他类型的药物,如肥大细胞稳定剂酮替芬和5HT-4受体激动剂普鲁卡必利,据报道可改善术后胃肠功能,但仍处于亚临床探索阶段[8, 9]。目前非药物疗法包括微创手术方式(腹腔镜)、嚼口香糖(包括尼古丁口香糖)、术后多模式镇痛等均有一定防治POI的作用,效果同样有限。
因此,无论是PONV还是POI,药物防治效果已经达到了瓶颈,需要有效的非药物防治手段作为补充。而以针灸为代表的穴位刺激在中国已经有数千年的应用历史,以其多靶点、效果确切、无毒副作用的优势逐渐成为防治POGD综合防治策略的重要补充。动物实验研究表明,针灸通过多靶点作用调节胃肠道功能,包括调节自主神经,抑制交感神经、兴奋副交感神经,促进胃肠蠕动及胃排空;通过作用于脑干,刺激介导NO、CCK-A受体和阿片类μ受体,引起食管下括约肌松弛率显着降低,抑制胃食管反流和胃肠逆蠕动;调节内源性大麻素系统,降低内脏敏感性;调节肠屏障,保护肠粘膜;刺激迷走神经,激活迷走神经抗炎通路等。此外,已经有充足的临床证据显示针灸可以改善胃肠道功能,疗效确切,安全无毒副作用。穴位刺激用以防治POGD具有较好的应用前景。因此本文制定穴位刺激防治POGD专家共识,为POGD的防治策略提供治疗方法的补充,并主要从PONV和POI两个方面的穴位刺激方案分别进行阐述。
穴位刺激方式的选择
穴位刺激防治PONV
根据十二经脉辩证,PONV的病机在于胃失和降、胃气上逆,临床特征为饮食、痰涎等胃内之物从胃中上涌,自口而出。防治PONV选穴原则以局部选穴、循经选穴、特定穴选穴为主。多选取具有调理脾胃功效的特定穴,内关(PC6)、足三里(ST36)是最常用腧穴,在选穴所属经脉上,主要集中于手厥阴心包经、足阳明胃经腧穴,在选穴部位上,主要在上肢部、下肢部、胸腹部的腧穴[12]。
PC6是目前公认的用于预防PONV的标准穴位[13](高质量,强推荐)。PC6属手厥阴心包经,通于任脉,会于阴维,联络上、中、下三焦,与三焦经互为表里,故PC6可以宣通上下,和胃降逆止呕。《灵枢·经脉》认为该穴位有补益气血,理气健脾,和胃降逆止呕的作用[14]。其位于腕臂内侧,掌长肌腱与桡侧腕。屈肌腱之间,腕横纹上2寸处[15]。PC6刺激预防PONV效果与抗呕吐药物(甲氧鲁普胺、苯甲嗪、普鲁氯嗪、氟哌利多、昂丹司琼、地塞米松)干预相当[13] [16](中质量,弱推荐)。PC6联合抗呕吐药物可降低术后呕吐发生率,但未降低术后恶心发生率(低质量,弱推荐)[13]。PC6联合其他穴位防治PONV效果更好,常用的配伍穴位有ST36、合谷(LI4)、耳穴神门(TF4)、天枢(ST25)、中脘(RNl2)、太冲(LR3)、上巨虚(ST37)、三阴交(SP6)等[12]。
ST36属足阳明胃经(多气多血,属胃络脾),是胃经的合穴及下合穴,土经的土穴。可治疗脾胃病如胃痛、呕吐、腹胀、消化不良、泄泻、便秘、痢疾、疳积,健身益体、预防中风等,是人体的保健要穴。由于其作用广泛,常需与其他穴位配伍达到具体防治某项疾病的效果。其位于小腿前外侧,犊鼻下3寸,距胫骨前缘外侧一横指(中指)。针刺ST36有调节机体免疫力、增强抗病能力、调节胃肠运动的作用,可使胃液总酸度和游离酸度趋于正常。现代研究发现,PC6、ST36对胃肠功能具有调节作用可能与下丘脑室旁核中存在同时对胃扩张刺激和针刺刺激起反应的躯体内脏汇聚神经元有关[17]。PC6配合ST36可增强调和气血、健脾和胃、降逆止呕之功效。腹腔镜胃癌根治术刺激PC6、ST36可显著降低PONV发生率,减少术后早期疼痛及止痛用量,缩短排气排便时间,促进胃肠功能的恢复,提高患者满意度[18]。剖宫产手术腰麻前30min刺激PC6、ST36可减低术中及术后恶心呕吐,提高产妇满意度[19]。
LI4属手阳明大肠经,根据中医的藏象学说及脏腑别通理论,“肝与大肠通”,取合谷穴可治疗与肝横犯胃引起的腹痛、呕吐等相关疾病(中等质量等级,强推荐)。其位于手背第一、二指骨间,当第二掌骨桡侧的中点处。现代研究证明,针刺LI4可增强胃肠蠕动,纠正胃总酸度、蛋白酶偏低,进而起到调整消化系统作用。LI4通常联合PC6防治PONV。研究显示:联合刺激PC6、LI4较单独刺激PC6效果更好,更能降低PONV的发生[20]。头颈部肿瘤切除术中联合刺激PC6、LI4可降低PCIA中曲马多所致的PONV[21]。妇科腔镜手术电针刺激PC6、LI4联合静脉注射托烷司琼对PONV的预防效果优于单纯静脉注射或单纯电针刺激[22]。
对于穴位刺激干预的最佳时间目前学术界存在争议,尚无统一标准。许多学者认为呕吐中枢CTZ能感受体液的化学刺激且一旦CTZ被激活,则不容易使其活性降低,且与恶心呕吐关系密切的5-HT在术中已经大量释放,因此主张在术前进行针刺治疗[23]。多项研究表明术前开始进行穴位刺激,对防治PONV有明显效果[24]。腹腔镜手术于术前或PACU苏醒时行低频电刺激15 min能显著减低PONV发生率,且术前刺激较术后刺激更有效[25]。直肠癌根治术分别于诱导前、切皮时及手术结束时予电针刺激30 min,结果显示术前针刺经穴可降低直肠癌根治术患者PONV的发生[26]。但也有研究显示术后开始针刺干预亦能有效防治PONV[27]。妇产科手术在手术结束时开始刺激PC6直至术后12 h,可预防PONV并增加患者舒适度[28]。腹腔镜胆囊切除术手术结束前5-10 min开始刺激PC6直至术后9 h,可减轻术后恶心,但不能减少术后呕吐[29]。
因此,对于手术时间在1 h内的短小手术,建议选择在麻醉诱导前30 min或诱导结束后开始,直至手术结束(高质量等级,强推荐)。对于时间较长的手术在手术苏醒前、苏醒回病房后可根据患者自身情况继续给予刺激(中等证据等级,弱推荐)。
上腹部手术,皮内针刺激T9-L3脊柱旁2.5cm的肝俞(BL18)、胆俞(BL19)、脾俞(BL20)、胃俞(BL21)、三焦俞(BL22)、肾俞(BL23)、气海俞(BL24),下腹部手术,皮内针刺激T11-L5脊柱旁2.5cm的脾俞(BL20)、胃俞(BL21)、三焦俞(BL22)、肾俞(BL23)、气海俞(BL24)、大肠俞(BL25)、关元俞(BL26),从麻醉诱导前2h开始刺激,进针5mm,留针至术后4天,较未刺激组术后恶心的发生率降低了20-30%[30]。腹腔镜手术电刺激PC6,其疗效与4mg昂丹司琼相当,且二者联合应用PONV发生率降低13%[16]。腹腔镜胆囊切除术,手术结束时行经皮神经电刺激(TENS),采用5Hz,电流强度在0.5-4mA之间,刺激颈部及乳突区神经至术后6h,结果显示前庭系统的电刺激对预防PONV有效 [31]。
建议:腹部手术如胆囊切除术,胃癌、结直肠癌根治术,单独刺激PC6或联合LI4、ST36可减低PONV发生率。
证据等级:高
推荐强度:强
妇科手术术前或术后按压或电刺激PC6 12-24h可降低PONV发生率[28, 32]。子宫切除术电针分别于术后5h、23h、47h刺激双侧PC6、ST36、上巨虚(ST37),能有效降低PONV发生率13-20%,同时可降低胃动素,升高血清胃泌素,改善胃肠功能[33]。剖宫产手术腰麻前30min单独刺激PC6或联合 ST36,可改善产妇术中及术后恶心呕吐,其机制与降低血浆5-HT浓度有关。[19, 34]
建议:妇科手术予诱导前地塞米松4mg及手术结束前托烷司琼2mg,并联合刺激(如电针、TEAS、佩戴ReliefBand及按压手环)PC6可进一步降低PONV发生率。
证据等级:高
推荐强度:强
麻醉诱导前或手术结束后电单独刺激PC6或联合LI4,可预防PONV,与昂丹司琼联用可进一步降低PONV发生率[36]。
建议: PC6刺激(如TEAS、佩戴ReliefBand)可与昂丹司琼联合应用预防PONV。
证据等级:高
推荐强度:强
麻醉诱导后手针刺激PC6、上脘(RN13),留针15min-20min,患儿术后呕吐发生率降低,与单用地塞米松无差异[38, 39]。电针刺激双侧PC6,麻醉苏醒后予4 Hz低频电刺激20min,可降低患儿术后恶心的发生,但未降低呕吐的发生及减少止吐药物的应用[40]。
建议:可在诱导后单独刺激PC6或联合RN13降低患儿术后恶心的发生。
证据等级:高
推荐强度:弱
神经外科手术,麻醉诱导前30min行TEAS,采用2/100Hz的疏密波,电流强度2mA,刺激单侧PC6至术后24h,较对照组可显著降低PONV发生率[41, 42]。心脏手术,手针刺激PC6、公孙(SP4)、三阴交(SP6)、神门(HT7)、内庭(ST44),从术前30min至3h开始刺激,留针20min,较未干预组可减低术后恶心的发生率及严重程度[43]。胸腔镜肺叶切除术,麻醉诱导前30min行TEAS,采用100Hz的密波刺激患侧PC6、LI4、列缺(LU7)、曲池(LI11)至手术结束,术后24h和48h各刺激30min,较对照组可降低PONV发生率[44]。刺激双侧PC6、LI4、后溪(SI3)、支沟(SJ6),对预防PONV有效[45]。
建议:其他手术类型可单独刺激 PC6或联合其他相关穴位降低PONV发生率,手针、电针、TEAS、佩戴ReliefBand均可应用。
证据等级:高
推荐强度:强
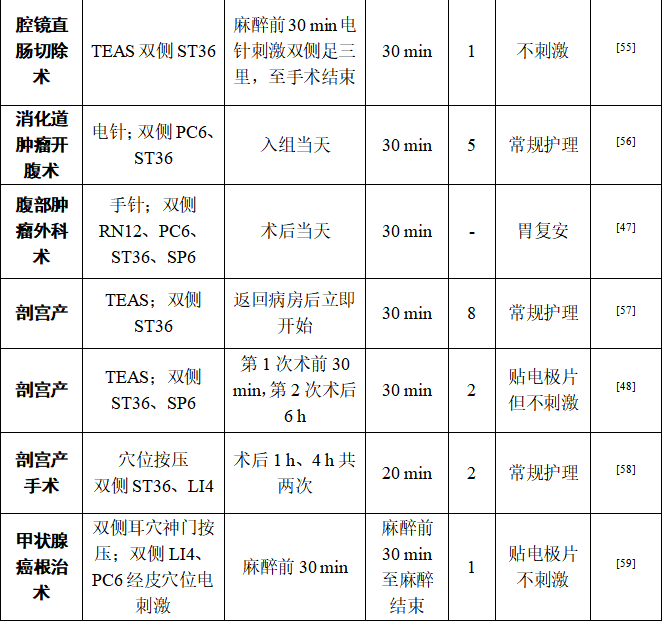
表1. 穴位刺激防治PONV操作推荐
穴位刺激防治POI
表2. 穴位刺激防治POI操作推荐
总结
穴位刺激防治POGD的有效性逐渐被临床所认可。无论是传统手针,还是电针、TEAS,都显示出可以多靶点、安全有效调控胃肠道功能的优势。随着ERAS理念的普及,穴位刺激有望配合药物疗法,进一步降低POGD的发生,加速患者术后康复。但距离穴位刺激在临床上广泛应用和普及还有很长的路要走。首先是目前关于穴位刺激的相关研究异质性较,如穴位配伍的方案不统一、穴位刺激方式也在不断地发展和更新,未来需要建立指导关于针刺研究的标准方案。
总之,穴位刺激在改善术后胃肠功能方面有非常好的应用前景,值得临床的关注。
[参考文献]
[1]CHANDRAKANTAN A, GLASS P S. Multimodal therapies for postoperative nausea and vomiting, and pain [J]. British journal of anaesthesia, 2011, 107 Suppl 1(i27-40.
[2]DABBOUS A S, JABBOUR-KHOURY S I, NASR V G, et al. Dexamethasone with either granisetron or ondansetron for postoperative nausea and vomiting in laparoscopic surgery [J]. Middle East journal of anaesthesiology, 2010, 20(4): 565-70.
[3]KOVAC A L. Updates in the Management of Postoperative Nausea and Vomiting [J]. Adv Anesth, 2018, 36(1): 81-97.
[4]FARHADI K, CHOUBSAZ M, SETAYESHI K, et al. The effectiveness of dry-cupping in preventing post-operative nausea and vomiting by P6 acupoint stimulation: A randomized controlled trial [J]. Medicine (Baltimore), 2016, 95(38): e4770.
[5]LIU K, HSU C C, CHIA Y Y. The effective dose of dexamethasone for antiemesis after major gynecological surgery [J]. Anesthesia and analgesia, 1999, 89(5): 1316-8.
[6]VENARA A, NEUNLIST M, SLIM K, et al. Postoperative ileus: Pathophysiology, incidence, and prevention [J]. J Visc Surg, 2016, 153(6): 439-46.
[7]U T, L B, R K, et al. Systemic prokinetic pharmacologic treatment for postoperative adynamic ileus following abdominal surgery in adults [J]. Cochrane Database Syst Rev 2008, 1): CD004930.
[8]FO T, MR B, A L, et al. The role of mast cell stabilization in treatment of postoperative ileus: a pilot study [J]. The American journal of gastroenterology, 2009, 104(9): 2257-66.
[9]STAKENBORG N, LABEEUW E, GOMEZ-PINILLA P J, et al. Preoperative administration of the 5-HT4 receptor agonist prucalopride reduces intestinal inflammation and shortens postoperative ileus via cholinergic enteric neurons [J]. Gut, 2018, 68(8): 1406-16.
[10]LIU Y, MAY B H, ZHANG A L, et al. Acupuncture and Related Therapies for Treatment of Postoperative Ileus in Colorectal Cancer: A Systematic Review and Meta-Analysis of Randomized Controlled Trials [J]. Evid Based Complement Alternat Med, 2018, 2018(3178472.
[11]段海峰, 朱懿峰, 路志红, et al. 刺激内关穴和足三里穴防治术后恶心呕吐的研究进展 [J]. 国际麻醉学与复苏杂志, 2017, 38(2): 166-70.
[12]石云舟, 王富春. 针灸治疗术后恶心呕吐选穴规律 [J]. 吉林中医药, 2016, 36(4): 325-8.
[13]LEE A, CHAN S K C, FAN L T Y. Stimulation of the wrist acupuncture point PC6 for preventing postoperative nausea and vomiting [J]. Cochrane Database of Systematic Reviews, 2015, 11):
[14]APFEL C C, KINJO S. Acustimulation of P6: an antiemetic alternative with no risk of drug-induced side-effects [J]. Br J Anaesth, 2009, 102(5): 585-7.
[15]朱丹, 吕黄伟. P6刺激对术后恶心呕吐有效性的Meta分析 [J]. 中国循证医学杂志, 2010, 10(8): 923-31.
[16]COLOMA M, WHITE P F, OGUNNAIKE B O, et al. Comparison of acustimulation and ondansetron for the treatment of established postoperative nausea and vomiting [J]. Anesthesiology, 2002, 97(6): 1387-92.
[17]姝 陈, 雍春燕, 恒 陈, et al. 针刺胃扩张模型大鼠内关_足三里等穴位下丘脑室旁核相关神经元的反应 [J]. 中国组织工程研究, 18(5): 675-80.
[18]GU S, LANG H, GAN J, et al. Effect of transcutaneous electrical acupoint stimulation on gastrointestinal function recovery after laparoscopic radical gastrectomy – A randomized controlled trial [J]. European Journal of Integrative Medicine, 2019, 26(11-7.
[19]刘延莉, 王明山, 李秋杰, et al. 经皮穴位电刺激治疗剖宫产产妇恶心呕吐及对血浆5-HT浓度的影响 [J]. 中国针灸, 2015, 35(10): 1039-43.
[20]ALIZADEH R, ESMAEILI S, SHOAR S, et al. Acupuncture in preventing postoperative nausea and vomiting: efficacy of two acupuncture points versus a single one [J]. Journal of acupuncture and meridian studies, 2014, 7(2): 71-5.
[21]ZHENG L H, SUN H, WANG G N, et al. Effect of transcutaneous electrical acupoint stimulation on nausea and vomiting induced by patient controlled intravenous analgesia with tramadol [J]. Chin J Integr Med, 2008, 14(1): 61-4.
[22]于艳宏, 陈宁. 电针刺激预防妇科腹腔镜术后恶心呕吐效果的观察 [J]. 中国妇幼健康研究, 2016, 27(08): 1015-7.
[23]NOROOZINIA H, MAHOORI A, HASANI E, et al. The effect of acupressure on nausea and vomiting after cesarean section under spinal anesthesia [J]. Acta medica Iranica, 2013, 51(3): 163-7.
[24]YAO Y, ZHAO Q, GONG C, et al. Transcutaneous Electrical Acupoint Stimulation Improves the Postoperative Quality of Recovery and Analgesia after Gynecological Laparoscopic Surgery: A Randomized Controlled Trial [J]. Evid Based Complement Alternat Med, 2015, 2015(324360.
[25]LEE S, LEE M S, CHOI D H, et al. Electroacupuncture on PC6 prevents opioid-induced nausea and vomiting after laparoscopic surgery [J]. Chin J Integr Med(1346), 2013, 19(4): 277-81.
[26]姚新宇, 杨华, 田小林, et al. 不同时机针刺经穴对直肠癌根治术患者术后恶心呕吐发生的影响:血浆胃泌素浓度的测定 [J]. 中华麻醉学杂志, 2012, 32(7): 820-3.
[27]WHITE P F, HAMZA M A, RECART A, et al. Optimal timing of acustimulation for antiemetic prophylaxis as an adjunct to ondansetron in patients undergoing plastic surgery [J]. Anesthesia and analgesia, 2005, 100(2): 367-72.
[28]ÜNüLü M, KAYA N. The Effect of Neiguan Point (P6) Acupressure With Wristband on Postoperative Nausea, Vomiting, and Comfort Level: A Randomized Controlled Study [J]. Journal of perianesthesia nursing : official journal of the American Society of PeriAnesthesia Nurses(0748), 2018, 33(6): 915-27.
[29]ZARATE E, MINGUS M, WHITE P F, et al. The use of transcutaneous acupoint electrical stimulation for preventing nausea and vomiting after laparoscopic surgery [J]. Anesthesia and analgesia, 2001, 92(3): 629-35.
[30]PHILIP E. Preoperative intradermal acupuncture reduces postoperative pain, nausea and vomiting, analgesic requirement and sympathoadrenal responses [J]. Journal of the Neurological Sciences(2448), 2013, 333(e520.
[31]CEKMEN N, SALMAN B, KELES Z, et al. Transcutaneous electrical nerve stimulation in the prevention of postoperative nausea and vomiting after elective laparoscopic cholecystectomy [J]. J Clin Anesth, 2007, 19(1): 49-52.
[32]FREY U H, SCHARMANN P, LOHLEIN C, et al. P6 acustimulation effectively decreases postoperative nausea and vomiting in high-risk patients [J]. Br J Anaesth, 2009, 102(5): 620-5.
[33]白红梅, 孙建华, 张杰. 电针联合托烷司琼预防全子宫切除术后恶心呕吐的效果 [J]. 临床麻醉学杂志, 2012, 28(12): 1158-60.
[34]EL-DEEB A M, AHMADY M S. Effect of acupuncture on nausea and/or vomiting during and after cesarean section in comparison with ondansetron [J]. Journal of anesthesia, 2011, 25(5): 698-703.
[35]HARMON D, RYAN M, KELLY A, et al. Acupressure and prevention of nausea and vomiting during and after spinal anaesthesia for caesarean section [J]. Br J Anaesth, 2000, 84(4): 463-7.
[36]GAN T J, JIAO K R, ZENN M, et al. A randomized controlled comparison of electro-acupoint stimulation or ondansetron versus placebo for the prevention of postoperative nausea and vomiting [J]. Anesth Analg, 2004, 99(4): 1070-5, table of contents.
[37]WHITE PAUL F, PH.D., M.D., ISSIOUI T, M.D., HU J, M.D., et al. Comparative Efficacy of Acustimulation (ReliefBand®) versus Ondansetron (Zofran®) in Combination with Droperidol for Preventing Nausea and Vomiting [J]. Anesthesiology: The Journal of the American Society of Anesthesiologists, 2002, 97(5): 1075-81.
[38]SOMRI M, VAIDA S J, SABO E, et al. Acupuncture versus ondansetron in the prevention of postoperative vomiting. A study of children undergoing dental surgery [J]. Anaesthesia, 2001, 56(10): 927-32.
[39]MOEEN S M. Could acupuncture be an adequate alternative to dexamethasone in pediatric tonsillectomy? [J]. Paediatric anaesthesia, 2016, 26(8): 807-14.
[40]RUSY L M, HOFFMAN G M, WEISMAN S J. Electroacupuncture prophylaxis of postoperative nausea and vomiting following pediatric tonsillectomy with or without adenoidectomy [J]. Anesthesiology, 2002, 96(2): 300-5.
[41]XU M, ZHOU S J, JIANG C C, et al. The effects of P6 electrical acustimulation on postoperative nausea and vomiting in patients after infratentorial craniotomy(3.248) [J]. Journal of neurosurgical anesthesiology, 2012, 24(4): 312-6.
[42]WANG X Q, YU J L, DU Z Y, et al. Electroacupoint stimulation for postoperative nausea and vomiting in patients undergoing supratentorial craniotomy [J]. Journal of neurosurgical anesthesiology, 2010, 22(2): 128-31.
[43]KORINENKO Y, VINCENT A, CUTSHALL S M, et al. Efficacy of Acupuncture in Prevention of Postoperative Nausea in Cardiac Surgery Patients [J]. Annals of Thoracic Surgery, 2009, 88(2): 537-42.
[44]HUANG S, PENG W P, TIAN X, et al. Effects of transcutaneous electrical acupoint stimulation at different frequencies on perioperative anesthetic dosage, recovery, complications, and prognosis in video-assisted thoracic surgical lobectomy: a randomized, double-blinded, placebo-controlled trial [J]. Journal of anesthesia, 2017, 31(1): 58-65.
[45]李晓曦, 陈冀衡, 范志毅, et al. 经皮多穴位电刺激对预防胸腔镜下肺叶切除术患者术后恶心呕吐的影响 [J]. 临床麻醉学杂志, 2016, 32(4): 333-6.
[46]HOU L, XU L, SHI Y, et al. Effect of electric acupoint stimulation on gastrointestinal hormones and motility among geriatric postoperative patients with gastrointestinal tumors [J]. Journal of traditional Chinese medicine = Chung i tsa chih ying wen pan, 2016, 36(4): 450-5.
[47]SUN B M, LUO M, WU S B, et al. Acupuncture versus metoclopramide in treatment of postoperative gastroparesis syndrome in abdominal surgical patients: a randomized controlled trial [J]. Zhong xi yi jie he xue bao = Journal of Chinese integrative medicine, 2010, 8(7): 641-4.
[48]ZHOU D, HU B, HE S, et al. Transcutaneous Electrical Acupoint Stimulation Accelerates the Recovery of Gastrointestinal Function after Cesarean Section: A Randomized Controlled Trial [J]. Evid Based Complement Alternat Med, 2018, 2018(7341920.
[49]HE D, WANG F Z, ZHANG Z, et al. Effect of low-frequency electrical acupoint stimulation on gastrointestinal motility function following radical gastrectomy in patients with gastric cancer [J]. Zhen ci yan jiu = Acupuncture research, 2020, 45(1): 51-6.
[50]ABADI F, SHAHABINEJAD M, ABADI F, et al. Effect of Acupressure on Symptoms of Postoperative Ileus After Cesarean Section [J]. Journal of acupuncture and meridian studies, 2017, 10(2): 114-9.
[51]BEN-ARIE E, KAO P Y, HO W C, et al. Acupuncture effect on digestion in critically ill postoperative oral and hypopharyngeal cancer patients: A protocol for double-blind randomized control trial [J]. Medicine (Baltimore), 2019, 98(35): e16944.
[52]DENG G, WONG W D, GUILLEM J, et al. A phase II, randomized, controlled trial of acupuncture for reduction of Postcolectomy Ileus [J]. Ann Surg Oncol, 2013, 20(4): 1164-9.
[53]HSIUNG W T, CHANG Y C, YEH M L, et al. Acupressure improves the postoperative comfort of gastric cancer patients: A randomised controlled trial [J]. Complementary therapies in medicine, 2015, 23(3): 339-46.
[54]HUANG W, LONG W, XIAO J, et al. Effect of electrically stimulating acupoint, Zusanli (ST 36), on patient's recovery after laparoscopic colorectal cancer resection: a randomized controlled trial [J]. Journal of traditional Chinese medicine = Chung i tsa chih ying wen pan, 2019, 39(3): 433-9.
[55]JIANG Q, MO Y C, JIN D, et al. Effect of acupoint stimulation on the quality of recovery in patients with radical thyroidectomy under the concept of enhanced recovery after surgery: a randomized controlled trial [J]. Zhongguo zhen jiu = Chinese acupuncture & moxibustion, 2019, 39(12): 1289-93.
[56]KIM G. Electroacupuncture for postoperative pain and gastrointestinal motility after laparoscopic appendectomy (AcuLap): study protocol for a randomized controlled trial [J]. Trials, 2015, 16(461.
[57]LI J J, ZHAO W S, SHAO X M, et al. [Effect of Transcutaneous Electrical Acupoint Stimulation on Post-surgical Gastrointestinal Function, Autonomic Nerve Activities and Plasma Brain-gut Peptide Levels in Patients Undergoing Gastrointestinal Surgery] [J]. Zhen ci yan jiu = Acupuncture research, 2016, 41(3): 240-6.
[58]LIU M Y, WANG C W, WU Z P, et al. Electroacupuncture for the prevention of postoperative gastrointestinal dysfunction in patients undergoing vascular surgery under general anesthesia: study protocol for a prospective practical randomized controlled trial [J]. Journal of integrative medicine, 2014, 12(6): 512-9.
[59]MENG Z Q, GARCIA M K, CHIANG J S, et al. Electro-acupuncture to prevent prolonged postoperative ileus: a randomized clinical trial [J]. World J Gastroenterol, 2010, 16(1): 104-11.
[60]MU L, GAO H, ZHAO M L, et al. Effect of transcutaneous electrical acupoint stimulation on recovery of gastrointestinal function after cesarean section [J]. Zhongguo zhen jiu = Chinese acupuncture & moxibustion, 2019, 39(3): 259-62.
[61]PAN H, LI J, ZHAO Y, et al. A Randomized Controlled Clinical Trial for Electroacupuncture Treatment of Post-surgical Gastrointestinal Dysfunction in Patients Undergoing Laparotomy [J]. Zhen ci yan jiu = Acupuncture research, 2016, 41(5): 457-61.
[62]TAN Y, ZHAO Y, HE T, et al. Efficacy and safety of auricular point acupressure treatment for gastrointestinal dysfunction after laparoscopic cholecystectomy: study protocol for a randomized controlled trial [J]. Trials, 2016, 17(1): 280.
来源:中华麻醉在线
版权归中华医学会麻醉学分会所有
不感兴趣
看过了
取消

人点赞

人收藏

打赏
不感兴趣
看过了
取消
©2012-2023 北京华媒康讯信息技术股份有限公司 All Rights Reserved. 注册地址:北京 联系电话:010-82736610
广播电视节目制作经营许可证 —(京)字第 17437号 京海食药监械经营备20200522号
京ICP备12011723号 京ICP证150092号
 京公网安备 11010802020745号
工商备案公示信息
互联网药品信息服务资格证书((京)-非经营性-2020-0015)
京公网安备 11010802020745号
工商备案公示信息
互联网药品信息服务资格证书((京)-非经营性-2020-0015)






您已认证成功,可享专属会员优惠,买1年送3个月!
开通会员,资料、课程、直播、报告等海量内容免费看!

打赏金额
认可我就打赏我~
1元 5元 10元 20元 50元 其它
打赏作者
认可我就打赏我~
扫描二维码
立即打赏给Ta吧!
温馨提示:仅支持微信支付!
已收到您的咨询诉求 我们会尽快联系您





































 010-82736610
010-82736610
 股票代码: 872612
股票代码: 872612




