
根据细胞因子谱类鉴别革兰氏菌指导抗生素使用治疗的有效率与广谱覆盖组接近,高达85%,而经验治疗组的治疗有效率仅为60%。
1、细胞因子与炎症
(1)预警细胞因子风暴,及时治疗,提高重症患者生存率
脓毒症、重症感染、噬血细胞综合征、肿瘤免疫治疗、发热待查、罕见变异病毒感染或大手术患者均可引起细胞因子风暴。监测细胞因子可及时治疗,预警细胞因子风暴风险,提高患者治疗有效率[1-3]。
(2)区分细胞因子风暴的三种免疫状态SIRS、CARS和MARS,并指导临床治疗
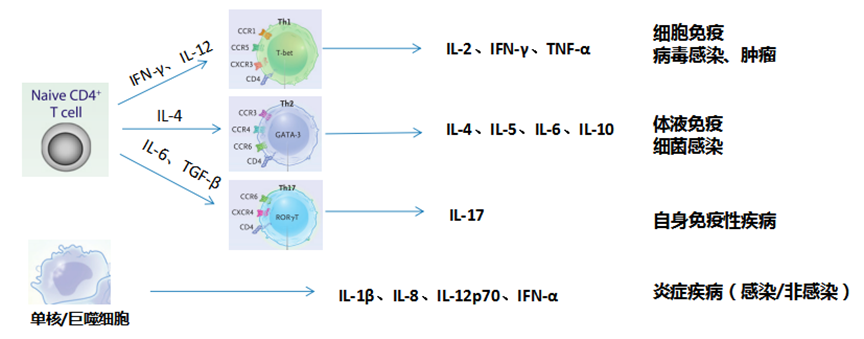
当感染或其他原因导致机体炎症反应失衡时,若大量促炎性因子如IL-1β、IL-6、IL-8、IL-12、IFN-γ、IFN-α及TNF-α水平大幅升高,有发生全身炎症反应综合征-SIRS风险,此时机体炎症反应强烈,建议进行抗炎治疗为主;若内源性抗炎反应过强,IL-4、IL-10等抗炎因子大幅升高,则提示CARS风险,此时机体的免疫功能比较弱,建议免疫增强治疗;若机体促炎因子和抗炎因子均大幅升高,则提示机体为混合性拮抗反应综合征,提示机体炎症反应强烈同时免疫功能低下,建议进行抗炎联合免疫增强治疗[2, 4-5]。
(3)诊断早期感染
IL-1β、IL-6、IL-8、TNF-α是普通感染患者主要升高的促炎因子;IFN-γ是病毒感染患者主要升高的细胞因子。细胞因子相比于传统的感染指标WBC、CRP、PCT窗口期更早,更有利于感染的早期诊断和指导治疗,提高治疗有效率;同时细胞因子半衰期更短,更有利于感染患者的药效监测[6-9]。
(4)细胞因子鉴别G-/G+菌感染
IL-6、IL-10同时升高大于10倍提示G-菌感染;IL-6升高2倍,IL-10升高倍增数小于10倍提示G+菌感染;根据细胞因子谱类鉴别革兰氏菌指导抗生素使用治疗的有效率与广谱覆盖组接近,高达85%,而经验治疗组的治疗有效率仅为60%[10]。
2、细胞因子与肿瘤
评估肿瘤微环境进展,辅助肿瘤早期诊断。若IL-6、IL-10、IL-12轻度升高,且IL-2、TNF-α、IFN-γ显著降低,提示可能有早期肿瘤微环境进展[11, 12]。预警PD-1治疗/CAR-T疗法不良反应细胞因子释放综合征(CRS)的发生[13]。
3、细胞因子与自身免疫性疾病
辅助诊断噬血细胞综合征:IL-6、IL-10、IFN-γ可区分噬血细胞综合征和脓毒症[14, 15]。辅助自身免疫病病情判断,监测免疫恢复情况[16-19]。
4、细胞因子的其他临床应用
辅助筛查流产病因,正常妊娠Th2 (IL-4、IL-10)激活,Th1 (IL-2、TNFα)抑制;复发性流产Th1上升,Th2下降,Th1/ Th2上升[20]。监测移植排斥与免疫,辅助早期干预治疗[21]。指导临床激素/抗炎药的应用。激素/抗炎药剂量过高易导致患者免疫功能低下,检测细胞因子可评估机体免疫功能,指导临床调整剂量,降低激素/抗炎药引发患者免疫低下导致继发感染的风险。
参考文献
[1]. 王仲等. 中国脓毒症早期预防与阻断急诊专家共识. 中国急救医学, 2020. 40(07): 577- 588.
[2]. Fajgenbaum, D.C. and C.H. June. Cytokine Storm. N Engl J Med, 2020. 383(23): 2255-2273.
[3]. Jekarl, D.W., et al.. Cytokine and molecular networks in sepsis cases: a network biology approach. Eur Cytokine Netw, 2018. 29(3): 103-111.
[4]. 中国医师协会急诊医师分会. 中国急诊感染性休克临床实践指南. 中华急诊医学杂志, 2016. 25(03): 274-287.
[5]. Hotchkiss, R.S., G. Monneret and D. Payen. Sepsis-induced immunosuppression: from cellular dysfunctions to immunotherapy. Nat Rev Immunol, 2013. 13(12): 862-874.
[6]. 刘又宁与解立新. 感染相关生物标志物临床意义解读专家共识. 中华结核和呼吸杂志, 2017. 40(04): 243-257.
[7]. Harbarth, S., et al.. Diagnostic value of procalcitonin, interleukin-6, and interleukin-8 in critically ill patients admitted with suspected sepsis. Am J Respir Crit Care Med, 2001. 164(3): 396-402.
[8]. Xu, X.J., et al.. Comparison of interleukin-6, interleukin-10, procalcitonin and C-reactive protein in identifying high-risk febrile illness in pediatric cancer patients: A prospective observational study. Cytokine, 2019. 116: 1-6.
[9]. Reinhart, K., M. Meisner and F.M. Brunkhorst. Markers for sepsis diagnosis: what is useful? Crit Care Clin, 2006. 22(3): 503-519.
[10]. Tang, Y., et al.. Th1/Th2 cytokine profiles in G+/G- bacteremia in pediatric hematology/oncology patients. Pediatr Blood Cancer, 2012. 58(1): 50-54.
[11]. Mantovani, A., et al.. Cancer-related inflammation. Nature, 2008. 454(7203): 436-444.
[12]. Lippitz, B.E.. Cytokine patterns in patients with cancer: a systematic review. Lancet Oncol, 2013. 14(6): e218-228.
[13]. Brudno, J.N. and J.N. Kochenderfer. Toxicities of chimeric antigen receptor T cells: recognition and management. Blood, 2016. 127(26): 3321-3330.
[14]. 噬血细胞综合征中国专家联盟与中华医学会儿科学分会血液学组. 噬血细胞综合征诊治中国专家共识. 中华医学杂志, 2018. 98(02): 91-95.
[15]. Xu, X.J., et al.. Diagnostic accuracy of a specific cytokine pattern in hemophagocytic lymphohistiocytosis in children. J Pediatr, 2012. 160(6): 984-990.
[16]. Ridgley, L.A., A.E. Anderson and A.G. Pratt. What are the dominant cytokines in early rheumatoid arthritis? Curr Opin Rheumatol, 2018. 30(2): 207-214.
[17]. Pacheco, Y., et al.. Cytokine and autoantibody clusters interaction in systemic lupus erythematosus. J Transl Med, 2017. 15(1): 239.
[18]. Talaat, R.M., et al.. Th1/Th2/Th17/Treg cytokine imbalance in systemic lupus erythematosus (SLE) patients: Correlation with disease activity. Cytokine, 2015. 72(2): 146-153.
[19]. Schulert, G.S. and A.A. Grom. Macrophage activation syndrome and cytokine-directed therapies. Best Pract Res Clin Rheumatol, 2014. 28(2): 277-292.
[20]. Yockey, L.J. and A. Iwasaki. Interferons and Proinflammatory Cytokines in Pregnancy and Fetal Development. Immunity, 2018. 49(3): 397-412.
[21]. Nomura, S., et al.. Can recombinant thrombomodulin play a preventive role for veno-occlusive disease after haematopoietic stem cell transplantation? Thromb Haemost, 2011. 105(6): 1118-1120.
文章来源:南京市第一医院医学检验科
编辑:青翠欲滴
校审:晨晨
不感兴趣
看过了
取消

人点赞

人收藏

打赏
不感兴趣
看过了
取消
©2012-2023 北京华媒康讯信息技术股份有限公司 All Rights Reserved. 注册地址:北京 联系电话:010-82736610
广播电视节目制作经营许可证 —(京)字第 17437号 京海食药监械经营备20200522号
京ICP备12011723号 京ICP证150092号
 京公网安备 11010802020745号
工商备案公示信息
互联网药品信息服务资格证书((京)-非经营性-2020-0015)
京公网安备 11010802020745号
工商备案公示信息
互联网药品信息服务资格证书((京)-非经营性-2020-0015)






您已认证成功,可享专属会员优惠,买1年送3个月!
开通会员,资料、课程、直播、报告等海量内容免费看!

打赏金额
认可我就打赏我~
1元 5元 10元 20元 50元 其它
打赏作者
认可我就打赏我~
扫描二维码
立即打赏给Ta吧!
温馨提示:仅支持微信支付!
已收到您的咨询诉求 我们会尽快联系您







































 010-82736610
010-82736610
 股票代码: 872612
股票代码: 872612




